Social Security Part B Employer Form

What Is Form W 2 W2 Forms Tax Forms Tax Return

Pin On Templates
Publication 957 01 2013 Reporting Back Pay And Special Wage Payments To The Social Security Administration Internal Revenue Service

Sample California Payroll Tax Form In 2020 Payroll Taxes Tax Forms Payroll

Cms L564 Request For Employment Information

Social Security Form Cms L564 Verifying Employment Information
Once section b has been completed by your employer return this form along with your part b application to your local social security office.
Social security part b employer form.

Pin On Template

Obamacare Tax Forms 1095 B And 1095 C 101 Tax Forms Tax Employer Identification Number

23 Cool Social Security Benefits Worksheet Photos Social Security Benefits Social Security Disability Benefits Social Security
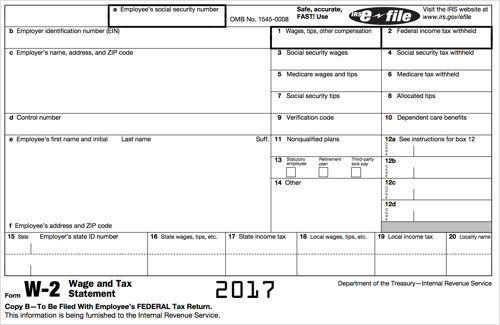
W 2 Form Smartasset

Application For Employment Pdf Resume Curriculum Vitae Cv Employment Application Job Application Template Job Application
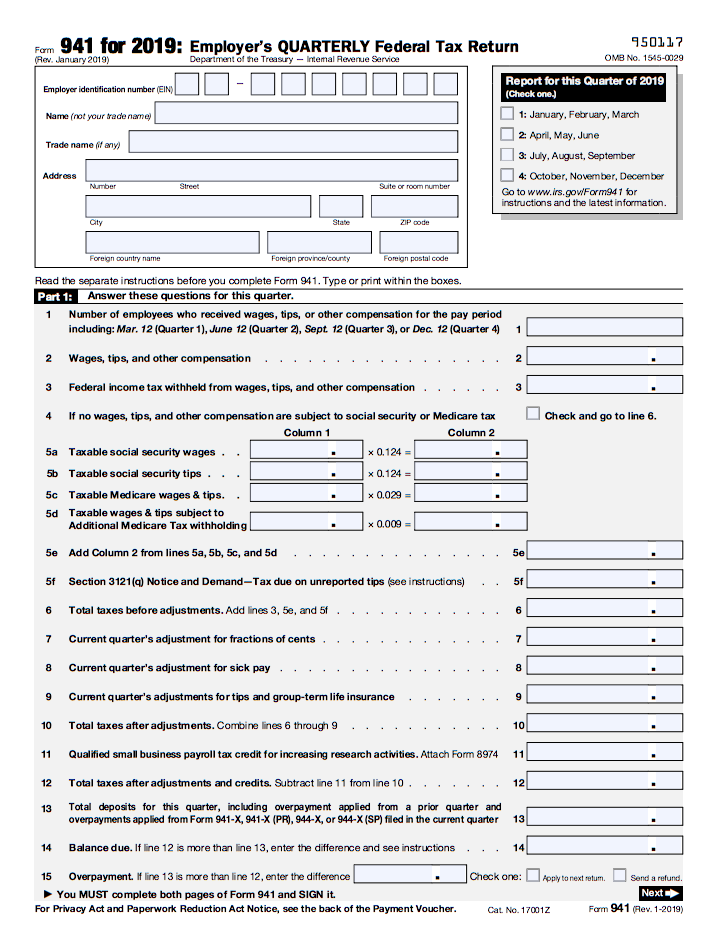
Form 941 Instructions How To File It Bench Accounting

F709 Generic3 Irs Forms Separation Agreement Template Irs

Fill Free Fillable Forms For The U S Social Security Administration
Understanding Your W 2 Controller S Office
Instant W2 Form Generator Create W2 Easily Form Pros

What Is A W 3 Form And How Do I File It Gusto

International Students And Social Security Numbers The Offiicial Flye Social Securty Disabilty Benifts About Retiering Years Medicaid And Mediplan Socia

Memo Onlyfans Creators Business Set Up And Tax Filing Tips Chris Whalen Cpa

Draft Of Revised Form 941 Released By Irs Includes Ffcra And Cares Provisions Current Federal Tax Developments

Installment Payment Plan Agreement Template Luxury Steps Forms To Prepare An Installment Agreement Contract Template How To Plan Income Based Repayment

Need A School Tax Form Templates Here S A Free Template Create Ready To Use Forms At Formsbank Com School Tuition Private School School Forms

Fillable W 4 Form Form W 4 In 2020 Tax Forms W4 Tax Form Need To Know

This Global Tax Software Report 2024 Focus On Global And Regional Market Providing Information On Major Players Like Manu Tax Software Marketing Global Prints
Https Encrypted Tbn0 Gstatic Com Images Q Tbn 3aand9gcqdy6iksxyglra4zfy9vu2acjfkqmkum5rdfg0bfv27enhz7dsv Usqp Cau

What Is The Process Of Claiming Worker S Compensation Workers Compensation Insurance Work Accident Compensation

Notice Of Reduced Earnings Fisherperson California Earnings First Names

1099 Form 2016 Download 1099 R Instructions For Recipient 2016 Printable Pdf In 2020 Form Job Application Form Irs Forms

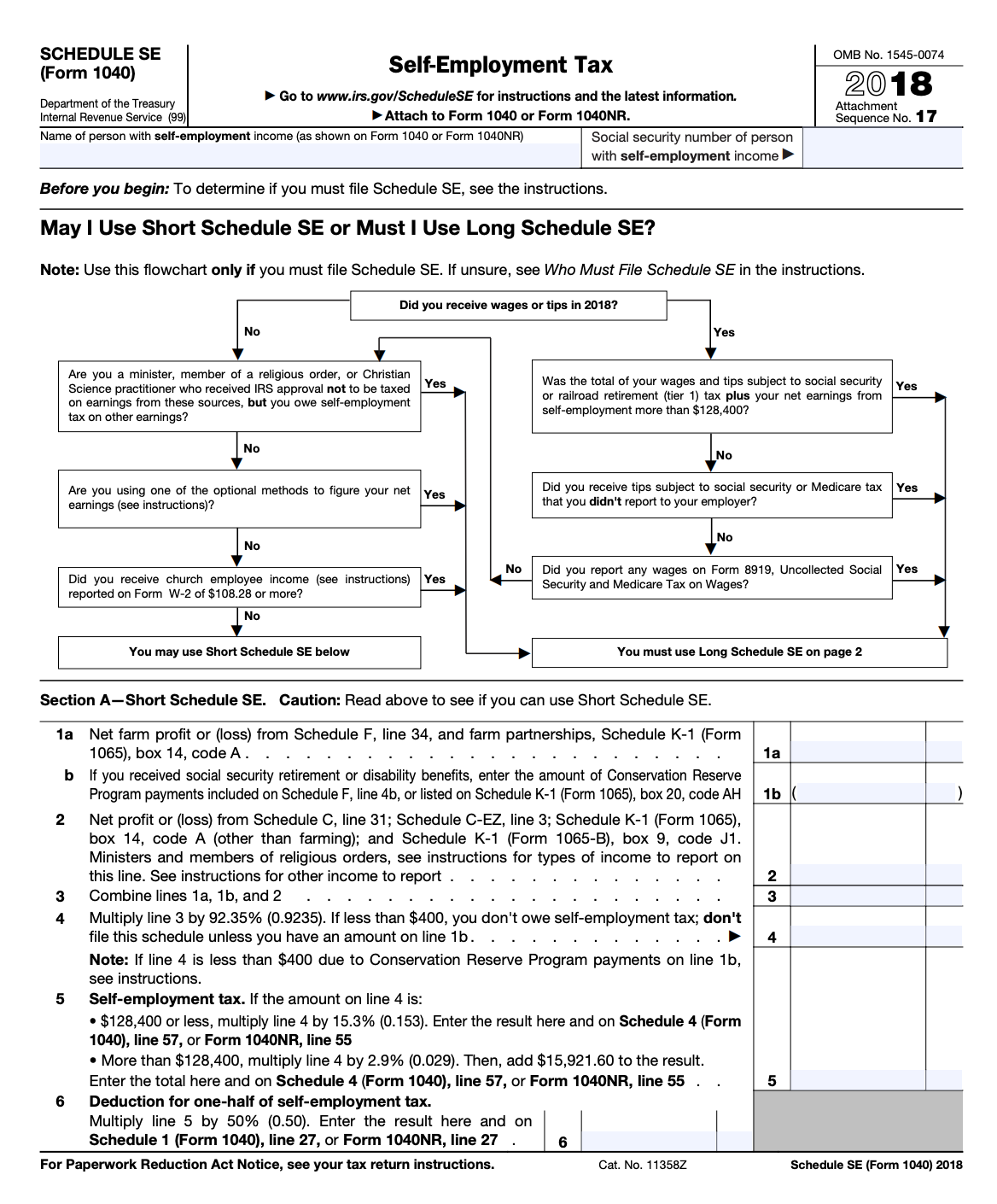
2017 Irs Tax Forms 1040 Schedule C Profit Or Loss From Business Irs Tax Forms Irs Forms Tax Forms

Freelance Taxes Income Writing Tips Freelance Writing Sole Proprietorship
Source : pinterest.com
